Hormone Changes After 40: How They Affect Your Weight
Before my 40s, I had no particular reason to think about hormone changes. The phrase “hormone changes after 40” appeared in health articles I scrolled past without much attention — it felt like a concern that belonged to someone else’s chart, not mine. I walked past health screening booths without stopping. Not out of fear — more a quiet assumption that there wasn’t much to find. My body felt fine. Life was busy. The thorough checkup could always happen later.
Then, somewhere in my early 40s, a few things shifted in ways I couldn’t quite name. My body started feeling heavier — not dramatically, just persistently, like something had been added that I couldn’t put down. I’d get dizzy on days when nothing in particular had changed. There were afternoons where getting through ordinary tasks required noticeably more effort than it should, a fatigue that didn’t lift the way it used to when I rested. I had not changed how I was living. Something else was changing.
I finally went for a proper checkup. My thyroid blood test came back within normal range. My doctor was about to move on — then paused and suggested an ultrasound as well. I hadn’t expected that. The ultrasound found two nodules.
I drove home with a printout I barely understood and a word I had not thought much about before: hormones. I knew the word existed. I had seen it in articles. But the hormone changes that happen after 40 had always felt like something for someone else’s medical chart — until that appointment made clear that they had been operating on mine, quietly, for some time already.
That was the beginning of a different kind of attention. The question that kept coming back was simple: I had not dramatically changed how I lived. So what had? What was happening inside that I hadn’t been watching?
This post is what I’ve learned since that appointment — what the specific hormone changes after 40 actually are, why they happen, what they do to weight and energy and body composition, and what the evidence supports in terms of responding to them intelligently rather than just trying harder at things that aren’t working.

📌 Hub Post — Explore the Full Topic
Why Hormones Override Calorie Logic After 40
The calorie model of weight management — eat less than you burn, lose weight — is not wrong. It describes basic physics. But it is radically incomplete as a practical tool for women in their 40s and 50s, because it treats the body as a static machine rather than a dynamic system running on hormonal instructions.
Hormones decide what happens to the calories you eat. They determine whether glucose gets burned for energy or stored as fat. Whether fat cells release their contents or hold them. Whether muscle tissue gets built or broken down. Whether you feel full after a meal or hungry an hour later. A calorie entering a body with balanced hormones is processed entirely differently from the same calorie entering a body with elevated cortisol, declining estrogen, and worsening insulin sensitivity.
This is the explanation for something that consistently baffles so many women in their 40s: eating less than ever and gaining weight anyway. The calories are not the problem. The hormonal instructions being sent to those calories have changed. And understanding which hormones are changing, and exactly how, is what makes it possible to respond in ways that actually address the problem.
📊 The Hormonal Shift After 40 — Key Numbers
Six hormonal shifts happen in the 40s and 50s that directly affect weight, body composition, energy, and appetite — and these hormone changes after 40 are the actual reason that diets and exercise routines that worked at 35 produce different results at 45. Some begin earlier than most women expect. Some interact with each other in ways that multiply their combined effect. And most of them are invisible until either a checkup reveals what’s changed, or the body starts behaving in ways that no longer respond to the usual approaches.
Estrogen: The Hormone Doing More Than You Realized
When I finally had my body composition measured — not just weight on a scale, but actual body fat percentage and muscle mass — I stood looking at those numbers for a long time.
My weight, to anyone looking at me, was unremarkable. I had been quite slim in my 20s and 30s, and even with the gradual gains of my early 40s, I fell somewhere within a normal range by standard charts. Nothing alarming. That is what made the composition numbers so disorienting. My body fat was well above average — pushing into the pre-obese category. My muscle mass was below average, close to the threshold for deficiency. The same body that looked normal from the outside had, internally, reorganized itself in a way I had not been watching.
“When did my muscles disappear?” I kept thinking. I had not stopped moving. I had not dramatically changed how I ate. I certainly had not been consuming the kind of diet that produces those numbers in a textbook. But the architecture of my body had been quietly shifting while I was paying attention to other things, and the numbers made that undeniable.
Estrogen is the primary driver of this shift — and it performs jobs that have nothing to do with reproduction that most women don’t know about until they’re gone. Before estrogen declines, it does three things simultaneously that directly affect body composition:
It supports insulin sensitivity — keeping cells responsive to insulin’s signal so glucose gets directed into cells for energy rather than converted to fat. It supports muscle protein synthesis — which is why muscle loss accelerates when estrogen falls, because the hormonal signal that helps maintain muscle tissue has diminished. And it regulates fat distribution — keeping fat stored preferentially in the hips, thighs, and the subcutaneous layer just under the skin, rather than in the visceral area deep in the abdomen.
As estrogen declines through perimenopause, all three weaken at once. Insulin sensitivity decreases. Muscle synthesis slows. Fat migration shifts from the periphery to the visceral region. The woman who finds herself at the same weight but a different shape — softer through the middle, less definition elsewhere — is watching exactly this process play out in her own body.
Visceral fat adds another layer of difficulty because it is not passive storage. It produces inflammatory compounds that further disrupt insulin signaling and actively contribute to its own expansion. The belly fat that appears in the 40s is not simply there — it is sustaining the hormonal conditions that keep it there.
✅ Addressing Estrogen-Driven Changes
- Resistance training 3×/week — the most powerful single intervention for both visceral fat and the insulin resistance that estrogen decline creates; also directly counteracts muscle loss
- Phytoestrogens in the diet — flaxseeds, edamame, tempeh, and legumes provide plant-based estrogen precursors that modestly support the system as natural estrogen declines
- Anti-inflammatory eating — directly interrupts the inflammatory cycle that visceral fat sustains and amplifies
- HRT discussion with a doctor — for women with significant symptoms, current evidence on hormone replacement therapy is considerably more nuanced and favorable than its public reputation; worth a genuine, up-to-date conversation
Progesterone: Why Sleep Broke Before Anything Else Did
In most conversations about hormonal changes after 40, estrogen takes center stage. Progesterone gets mentioned afterward, briefly, as if it’s a secondary concern. But for many women, the symptoms that feel most disorienting in the early perimenopausal years — the ones that seem to come from nowhere and don’t quite fit a clear category — are progesterone symptoms. Progesterone begins declining first, often in the mid-to-late 30s, well before estrogen makes its more dramatic exit.
The place most women feel this first is sleep. Not the dramatic insomnia of not being able to fall asleep at all — more the quality of the sleep itself quietly degrading. Waking at 2 or 3am for no clear reason and lying there for an hour. Sleeping eight hours and feeling as if it was five. A persistent fatigue that doesn’t improve with more time in bed, because the sleep itself is no longer reaching the restorative depths it used to.
Progesterone promotes slow-wave sleep — the deep stages where growth hormone is released, cellular repair happens, and the nervous system actually recovers from the day. Without adequate progesterone, sleep becomes lighter and more fragmented. It’s technically happening, but the architecture has changed in ways that prevent it from doing its full restoration job.
Progesterone also supports the GABA pathway — the nervous system’s primary calming, inhibitory mechanism. When progesterone is adequate, it acts as a natural buffer on the stress response. As it declines, that buffer disappears. The result is often a low-grade baseline alertness that makes evenings harder to wind down from — not dramatic anxiety, just a heightened state that wasn’t there at 35 and now seems to be the default setting.
From a weight management perspective, the progesterone decline matters primarily through its effect on sleep — because disrupted sleep, as the leptin and ghrelin section will show, directly worsens hunger regulation, elevates cortisol, and creates the hormonal conditions for fat storage. Progesterone loss is often the first link in a chain that eventually touches everything else on this list.
On Magnesium and the GABA Pathway
Magnesium glycinate (300–400mg before bed) supports the GABA function that declining progesterone used to provide. It’s one of the more consistently useful supplemental approaches for the sleep disruption of perimenopause — not a replacement for progesterone itself, but a meaningful support for the same pathway. The glycinate form is significantly better absorbed than magnesium oxide and much less likely to cause digestive side effects.
Cortisol: Running Hotter Without Estrogen’s Guardrails
One of the more disorienting realizations of my 40s was that the same level of daily pressure that had felt manageable at 38 felt noticeably different at 44. Not because my life had dramatically changed — the work pressures, the household demands, the ongoing mental load were roughly the same. My capacity to process them without it registering physically seemed to have shrunk. The same inputs were producing a larger output.
The mechanism involves estrogen’s relationship with the HPA axis — the hypothalamic-pituitary-adrenal system that governs cortisol production. Estrogen moderates that system. It dampens cortisol spikes and, crucially, accelerates the recovery time after a stressor has passed. When estrogen is adequate, a difficult afternoon produces a cortisol response that climbs and then returns to baseline relatively quickly. When estrogen declines, the same stressor produces a larger cortisol elevation — and that elevation persists longer before resolving.
The consequences for body composition are direct and specific. Chronically elevated cortisol signals the body to store energy as visceral fat, preferentially in the abdominal region because that location is close to the liver — exactly where stored fuel can be rapidly mobilized if the stress turns out to require physical action. It breaks down muscle tissue for quick glucose, accelerating the muscle loss that estrogen decline has already started. It drives cravings for calorie-dense foods because the stressed body is actively searching for fast fuel. And it disrupts evening sleep by elevating baseline arousal at exactly the hours when cortisol should be dropping to allow sleep onset.
The Exercise Paradox After 40
- Long sustained cardio sessions significantly raise cortisol — and in the lower-estrogen environment of perimenopause, this elevation persists longer and does more metabolic damage than it did at 35
- Adding more intense cardio when weight loss stalls can actively worsen the cortisol environment driving belly fat accumulation
- The consistent research finding: shorter, smarter sessions (20–30 min resistance or interval training) rather than longer, harder ones for women in this hormonal environment
- Morning light exposure (10–15 min outdoors within an hour of waking) helps anchor the daily cortisol rhythm, supporting the natural decline through the day
Insulin: When the Same Foods Work Differently
The blood pressure reading from my checkup sat with me for days. Pre-hypertensive. My doctor had been direct: make dietary and lifestyle changes, or we would be talking about medication at the next visit. I had not expected that outcome — not because I was living carelessly, but because I was not. I was not someone who ate poorly by any obvious measure. The numbers felt disconnected from the life I was actually living.
What I did not understand then was that pre-hypertension and the body composition results I’d seen — elevated fat percentage, declining muscle — are frequently downstream of the same root cause: worsening insulin sensitivity driven by the estrogen decline that was already underway.
Insulin’s job is to move glucose from the bloodstream into cells after a meal. When cells are insulin-sensitive — as they tend to be in younger women with adequate estrogen — this system runs efficiently. Blood sugar rises, insulin is released, glucose enters cells, blood sugar normalizes. When cells become insulin-resistant, they stop responding to insulin’s signal with the same efficiency. The pancreas compensates by releasing more. The result is chronically elevated insulin — and elevated insulin, sustained over time, is a near-constant fat-storage signal that keeps fat cells in accumulation mode and prevents the body from accessing stored fat for energy in between meals.
The practical consequence most women notice first is that foods that used to feel neutral start producing visible effects — bloating, energy crashes, weight gain that seems disproportionate to what was actually consumed. The meal that felt unremarkable at 37 produces a different response at 45. This is not imagination or sensitivity. The insulin response to that same meal is measurably larger now, producing proportionally more fat storage from food that used to be metabolically unremarkable.
The blood pressure connection runs through the same pathway: chronic insulin elevation promotes sodium retention and alters blood vessel tone in ways that raise blood pressure over time. My checkup numbers were not separate problems. They were the same system, sending the same signal through different channels.
✅ Improving Insulin Sensitivity After 40
- Resistance training 3×/week — exercised muscle absorbs glucose directly and independently of insulin, essentially bypassing the broken signaling; the most powerful insulin-sensitizing intervention available short of medication
- 10-minute walk after meals — reduces post-meal glucose spike by up to 30% through direct muscle glucose uptake; one of the simplest and most underused metabolic tools available
- Vegetables and protein before carbohydrates — meal sequencing reduces peak blood sugar response by 20–30% from the exact same foods eaten in a different order
- Reduce ultra-processed carbohydrates — the foods producing the largest insulin spikes with the least nutritional return are the most efficient place to start
- Adequate sleep — even one week of 5–6 hour nights measurably worsens insulin sensitivity in healthy adults; sleep is not a lifestyle bonus, it’s a metabolic requirement
Thyroid: Numbers That Look Fine but Aren’t Fully Working
The two thyroid nodules found on my ultrasound sent me somewhere I had not expected to go. The nodules themselves were benign — small, without features that suggested urgency, to be monitored rather than immediately treated. But the finding opened a conversation about thyroid function that a normal blood panel result would never have prompted.
I had not been thinking about my thyroid before that checkup. I had not connected it to the heaviness I’d been feeling, the occasional dizziness, the fatigue that didn’t fully resolve with rest. The blood test had come back “within normal range,” and that phrase had almost ended the inquiry. The ultrasound changed the direction of the conversation — and with it, my understanding of what “normal range” actually means in the context of how a 40-something woman is actually functioning.
Thyroid nodules are more common than public awareness reflects. Research indicates they’re present in a meaningful percentage of adults, with prevalence rising with age — and they occur considerably more often in women than in men. Most are benign. But their presence is frequently a signal worth looking at more closely, because thyroid health and the hormonal transition of perimenopause are directly connected in ways that can produce genuine dysfunction while standard test results remain technically acceptable.
The thyroid regulates the metabolic rate of every cell in the body — how efficiently the gut moves, how quickly the liver processes other hormones, how clearly the brain runs, how many calories the body burns at rest just to sustain itself. When thyroid output slows even modestly, the entire system operates at a lower metabolic level that diet alone cannot compensate for. The fatigue that doesn’t lift with rest, the mental flatness that isn’t quite brain fog but isn’t quite sharp either, the weight that doesn’t respond proportionally to effort — these are the signatures of thyroid underperformance that can coexist with blood numbers that a doctor calls normal.
The perimenopause connection is direct: estrogen decline affects thyroid receptor sensitivity. Chronic cortisol interferes with the conversion of inactive T4 thyroid hormone into the active T3 form that cells actually use. The immune dysregulation that can accompany this transition raises the risk of autoimmune thyroid conditions. Women in their 40s are at a convergence point where several mechanisms can simultaneously reduce thyroid effectiveness — while TSH testing alone may show nothing actionable.
Getting a Complete Thyroid Picture
- Ask for a full panel, not just TSH: free T3, free T4, and TPO antibodies (thyroid peroxidase — detects Hashimoto’s autoimmune thyroiditis, which is significantly more common in women and frequently surfaces or worsens in the perimenopausal years)
- “Within normal range” paired with significant symptoms is a conversation to continue, not a conclusion — some clinicians consider TSH above 2.0–2.5 functionally suboptimal for symptomatic women
- Selenium supports the T4-to-T3 conversion that elevated cortisol disrupts — found in Brazil nuts (1–2 per day is sufficient), tuna, sardines, and eggs
- Adequate iodine is essential for thyroid hormone production — seaweed, seafood, dairy, and iodized salt are primary sources for most women
- Managing cortisol reduces one of the key mechanisms actively interfering with thyroid conversion; the two hormonal systems are not separate problems
For a thorough overview of thyroid conditions and what testing covers, the NIH’s thyroid disease resource is a reliable and comprehensive starting point.
Leptin and Ghrelin: Hunger Signals That Stopped Making Sense
At some point I noticed that I couldn’t fully trust my own sense of hunger and fullness anymore. Not in a dramatic way — just that the feedback was less reliable than it used to be. I’d finish dinner and feel plainly uncertain about whether I was satisfied. The signal that used to arrive clearly — that settled, complete feeling after a meal — had become harder to read.
I started experimenting with reducing my dinner portion, roughly cutting it by half. The first several evenings were uncomfortable. But something happened almost immediately that I hadn’t anticipated: my stomach felt noticeably more settled at bedtime. Not dramatically different, just quieter. Less active. That quieter stomach made falling asleep easier than it had been in a while. I found myself in bed earlier — not because I had decided to sleep earlier, but because the restless, slightly unsatisfied feeling that had been keeping me up simply wasn’t there.
Earlier to bed meant more sleep. More sleep meant mornings that felt completely different — clearer, more functional, with a quality of readiness that had been absent. Within a week or two, something else began to shift: my stomach started adapting. The urgent quality of evening hunger began to settle. A normal amount of food at dinner started feeling like enough. I began to understand, for the first time in a while, what it felt like to be physically light.
What I learned later was that this sequence — reduced dinner, improved sleep, changed hunger signals — maps directly onto the leptin and ghrelin system, and exactly what goes wrong with it in the hormonal environment of the 40s.
Ghrelin is the hunger signal: it rises before meals and should drop after eating. Leptin is the satiety signal: it rises with adequate fat stores and is supposed to tell the brain that energy reserves are sufficient and eating can stop. Together, these two hormones should create a reliable, self-regulating feedback loop. In the 40s, this loop becomes unreliable in two specific ways. Leptin resistance develops as visceral fat accumulates — the brain stops receiving the fullness signal clearly even though leptin itself is present. And ghrelin rises sharply in response to sleep deprivation, stress, and caloric restriction — all of which are increasingly common in women during this decade.
The urgent evening hunger, the dissatisfaction after a meal that was objectively sufficient, the cravings that arrive late at night as if no dinner happened — these are disrupted hormonal signals. The dinner experiment I did accidentally interrupted the cycle by improving sleep first, which reduced ghrelin, which made the hunger signals more proportionate, which made the feeling of fullness more accessible again. Sleep was the key that opened everything else.

How All Six Amplify Each Other
Looked at individually, each of these hormone changes after 40 is significant but manageable. The reason the 40s feel so different from earlier decades is that these changes rarely arrive one at a time. They interact — and the interactions amplify the individual effects in ways that make the combined picture considerably harder to address than any single piece of it.
Declining estrogen increases insulin resistance. Increasing insulin resistance drives more visceral fat accumulation. More visceral fat produces inflammatory compounds that further disrupt insulin signaling and also interfere with cortisol regulation. Declining progesterone fragments sleep. Fragmented sleep elevates cortisol. Elevated cortisol suppresses the T4-to-T3 thyroid conversion, reducing the metabolic rate that everything else depends on. It also worsens insulin resistance, depositing more visceral fat. Disrupted sleep raises ghrelin and blunts leptin sensitivity, producing hunger and cravings that make the dietary consistency required by all the other changes significantly harder to maintain.
This is the mechanism behind something that so often baffles women in this stage: doing everything correctly — eating well, exercising, sleeping reasonably — and still not seeing the body respond the way it used to. The system is not broken. It is interconnected in ways that require addressing multiple variables simultaneously rather than rotating through single-variable solutions one at a time.
The encouraging counterpart: the core interventions that support one of these hormones tend to support all of them. Resistance training improves insulin sensitivity, reduces visceral fat, supports sleep quality, and directly counteracts muscle loss — four different problems addressed by one consistent practice. Quality protein preserves muscle, stabilizes blood sugar, and supports satiety even when leptin resistance has weakened the primary fullness signal. Sleep is the most horizontal intervention available — it supports every hormone on this list simultaneously, in ways that nothing else replicates or substitutes for.
The system is interconnected, which means the response needs to be too. Not a comprehensive overhaul of everything at once — but a set of consistent foundations that address the actual mechanisms rather than their surface symptoms.
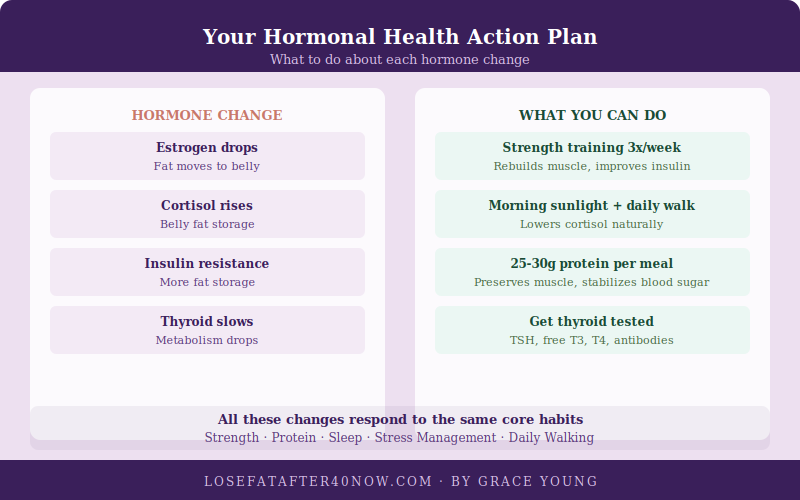
The Hormonal Action Plan — What the Evidence Supports
| Hormone | Key Change After 40 | Primary Response |
|---|---|---|
| Estrogen | Declines → visceral fat shift, insulin resistance, muscle loss | Resistance training, adequate protein, phytoestrogens |
| Progesterone | Declines first → fragmented sleep, low-grade anxiety, bloating | Magnesium glycinate, consistent sleep timing, stress reduction |
| Cortisol | Elevated longer without estrogen moderating it → belly fat, cravings, sleep disruption | Shorter smarter exercise, morning light, active recovery time |
| Insulin | Resistance increases → fat storage rises from carbohydrates | Resistance training, post-meal walking, meal sequencing |
| Thyroid | Output may slow → lower metabolic rate throughout | Complete panel testing, selenium, reduce cortisol interference |
| Leptin / Ghrelin | Signals disrupted → unreliable hunger and fullness feedback | Sleep quality, high-protein meals, avoid severe restriction |
The convergence across every row toward the same cluster of interventions — resistance training, adequate protein, quality sleep, and movement that manages rather than spikes cortisol — is not because this advice is formulaic. It’s because those four foundations address the actual biology of hormone changes after 40. They work at the level of the mechanism, not just the symptom.
Frequently Asked Questions
What are the earliest signs of hormone changes after 40?
For most women, the earliest signals are sleep-related — lighter sleep, waking in the early hours without clear cause, sleeping adequate hours but waking unrested. This typically reflects progesterone’s early decline, which begins before estrogen makes its more dramatic changes. Other early signs include bloating or fluid retention that seems disproportionate to food intake, a lower baseline energy that doesn’t respond to rest the way it used to, and a reduced stress resilience — the same demands feeling more taxing than they did a few years earlier. Weight changes and body composition shifts tend to become more noticeable later, once estrogen and insulin sensitivity changes have accumulated.
Is the weight gain from hormonal changes different from regular weight gain?
Yes, in location, composition, and response to standard interventions. Hormonal weight gain after 40 preferentially accumulates as visceral fat in the abdominal region — driven by estrogen decline and insulin resistance — rather than distributing more evenly as fat gain tended to earlier in life. It is also accompanied by simultaneous muscle loss, so the scale may show modest increases while body composition has shifted significantly. And it responds poorly to caloric restriction alone: cutting calories without addressing insulin resistance, cortisol, or muscle loss often produces metabolic adaptation without meaningful fat loss, which is why the approaches that worked at 35 frequently don’t work at 45.
Should I get hormone testing done, and what should I ask for?
If you’re experiencing unexplained weight gain, persistent fatigue that doesn’t respond to rest, sleep disruption, body composition changes that don’t respond to diet and exercise, or mood instability, a comprehensive panel is worth pursuing. At minimum, ask for: TSH plus free T3, free T4, and TPO antibodies for a complete thyroid picture; fasting insulin and glucose for insulin resistance; and if perimenopause symptoms are significant, estradiol and progesterone at the appropriate point in your cycle. Standard annual blood work often misses meaningful dysfunction — a “within normal range” result is a starting point for conversation, not necessarily a conclusion, particularly when significant symptoms are present.
Why does my body feel unfamiliar to me right now?
Because it has actually changed — not just in weight but in composition, distribution, and how it responds to the same inputs. The hormonal changes of this decade alter where fat is stored, how much muscle is maintained, how the body processes food, and how hunger and fullness are regulated. These are not the same as ordinary weight fluctuations experienced earlier in life, which is why the body can feel foreign in a way that’s different from just weighing more. Understanding what’s actually driving those changes — which hormones, and through what mechanisms — tends to reduce the distress significantly, because it reframes the experience from inexplicable personal failure to a biological transition with identifiable, addressable causes.
How long before lifestyle changes actually begin to shift the hormonal picture?
Different interventions work on different timelines. Sleep improvements from magnesium glycinate and environmental adjustments are often noticeable within one to two weeks. Post-meal blood sugar improvements from walking and meal sequencing are measurable almost immediately. Meaningful improvement in insulin sensitivity from consistent resistance training typically appears within six to eight weeks. The longer arc — improved cortisol regulation, visible changes in body composition, stabilization of hunger signals — tends to unfold over three to four months. This is also roughly the window where the compounding effect of multiple consistent changes begins to be visible and felt simultaneously, which is why the first two to three months often feel like slow progress before things start accelerating.
If one section of this explained something that’s been confusing about your own body, I’d really like to know which one in the comments. These are the conversations I wish I’d had access to much earlier — and each one helps someone else find it sooner.
Medical Disclaimer: This post is for informational purposes only and does not constitute medical advice. Please consult with a qualified healthcare provider for personalized guidance regarding hormonal health, testing, and any treatment options.
Grace Young is the founder of losefatafter40now.com. She spent years learning what was actually driving the changes in her own body — piecing together what no single appointment had fully explained — and has spent the years since sharing what actually helps, so other women don’t have to figure it out alone. Read Grace’s full story →




