Menopause Weight Gain: How to Fight It After 40 (Complete Guide)
At 43, I wasn’t worried about menopause weight gain. I was exercising the way I always had, eating the way I always had, and the number on the scale barely crossed my mind. When it crept up a pound or two that year, I assumed it was temporary. My body had corrected itself before.
At 44, I opened my food-tracking app one evening out of habit rather than concern. The amount I was eating hadn’t changed. My workouts hadn’t changed. But the weight graph kept climbing, slowly, month after month. I told myself the same thing I’d told myself a dozen times before: this will level out on its own. So I didn’t change anything.
Then I turned 45, and pulled up that same app to check something unrelated. I sat there for a long moment doing the math. Eleven point four pounds heavier than I’d been at 43. Not from a single bad month. Not from one holiday season I could blame. Two years of doing exactly what I’d always done, and my body had responded in a way it never had before.
That was the first time I asked myself a question I’d never needed to ask in my thirties: what if the problem isn’t something I’m doing wrong, but something in my body that’s working differently now?
Menopause weight gain is real, it’s documented, and it isn’t a character flaw or a motivation problem. It’s the result of several physiological shifts happening at once, and understanding those shifts is what actually changes what you do next.

Menopause Weight Gain: The 5 Mechanisms Behind It
Menopause weight gain isn’t one problem with one cause. It’s five separate physiological changes landing at roughly the same time, which is part of why it can feel so disorienting. You haven’t changed anything, and your body is responding to the transition itself.
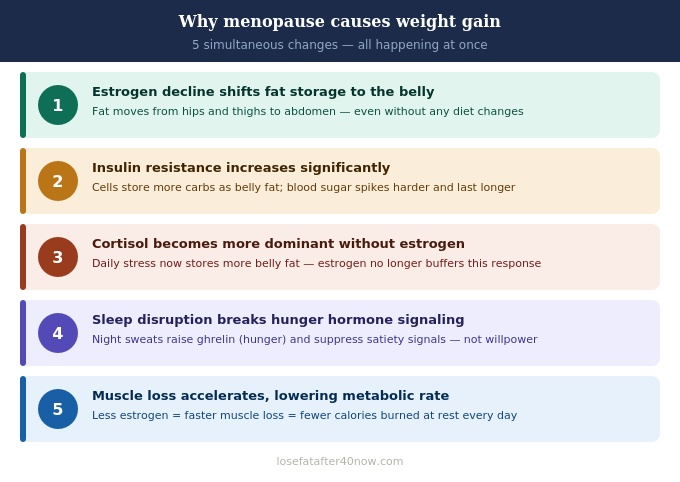
Before menopause, estrogen favors fat storage in the hips and thighs. As estrogen drops, storage shifts toward the abdomen, including visceral fat, the deep fat that surrounds your organs. This shift happens independently of how much you’re eating. It’s a hormonal redirection, not a behavioral one.
Estrogen plays a direct role in how sensitive your cells are to insulin. As it declines, that sensitivity drops, so more of what you eat gets stored as fat rather than used for immediate energy. This mechanism, and the specific role estrogen plays in it, is covered in full in our guide on estrogen and weight gain.
Estrogen normally softens the fat-storing effects of cortisol, your stress hormone. Without that buffer, ordinary daily stress produces a stronger abdominal fat response than it used to. The full mechanism behind this, including why cardio can sometimes make it worse instead of better, is in our cortisol guide.
Night sweats and hormonal shifts fragment sleep during the menopausal transition. The next day, ghrelin, your hunger hormone, runs higher, while the hormone responsible for feeling satisfied after eating runs lower. You end up hungrier and less satisfied, and it has nothing to do with willpower.
Estrogen supports muscle protein synthesis. As it declines, muscle loss accelerates well beyond the gradual rate you’d expect from aging alone. Less muscle means a lower resting metabolic rate, which means the same calories that once maintained your weight now add to it.
I didn’t notice any of this through a scale first. I noticed it through a jacket.
Fall arrived and I pulled out a jacket I hadn’t worn since spring. The sleeves were looser than I remembered, if anything, my arms looked about the same as they always had. But the waist was tighter, in a way that had nothing to do with the pounds I already knew about.
Looking in the mirror, my arms and legs hadn’t really changed shape. My midsection had. That was more unsettling than the number on the scale, because it meant something more specific than “I gained weight.” It meant my body was storing fat in a place, and in a way, it never had before.
Where the Weight Actually Goes
Not all fat behaves the same way, and that distinction matters more after menopause than it did before.
| Subcutaneous Fat | Visceral Fat |
|---|---|
| Sits just under the skin (hips, thighs, arms) | Surrounds the organs deep in the abdomen |
| Responds fairly directly to diet and exercise | More resistant to general weight-loss effort alone |
| Relatively low metabolic activity | Metabolically active, releases inflammatory compounds |
| Was the dominant type of fat gain before menopause | Increases disproportionately during the menopausal transition |
This is why the number on the scale can stay fairly steady while your waistband tells a completely different story. Estrogen decline is directly linked to increased central fat distribution, independent of overall body weight (Mayo Clinic Proceedings, 2017). Your belly can feel firmer and more internal for a reason: that’s deep visceral tissue, not the softer subcutaneous fat you may be used to, and it typically needs a different combination of strategies to address.
For a long time, I assumed the fix for all of this was simply to work harder, so that’s what I did.
Before all this started, a hard workout would leave me tired for a day, maybe less. Somewhere in this transition, that changed. I’d wake up the morning after a workout still heavy with fatigue, and instead of clearing by the next afternoon, it would drag into a second day, sometimes a third.
My first assumption was that I simply needed to push through it, so I trained more often rather than less. Instead of bouncing back, my body felt increasingly weighed down, and the number on the scale refused to move in the direction I expected. That was the first real crack in the belief that more effort alone would solve this.
The Turning Point: What My HRT Consultation Actually Started With
Months into this, still waking up tired, still not seeing the changes I expected from consistent effort, I finally made an appointment with a menopause-focused specialist, prepared to talk about my weight.
That isn’t what the appointment led with. Before we discussed weight at all, she asked whether I was waking up during the night, whether I had night sweats, whether I felt hot or flushed unpredictably, and how tired I felt each morning regardless of how much sleep I’d logged.
I’d come in expecting a conversation about calories and expected to leave with a diet plan. Instead the conversation started with sleep and hormones, and it took me a moment to understand why that mattered. That was the moment I first considered that this might not be a discipline problem at all. It might be a hormonal one.
- Hormone therapy is primarily used to manage hot flashes and related symptoms, but it can also help redistribute the visceral fat that accumulates around the abdomen during menopause
- Because HRT often improves sleep quality, it can indirectly make lifestyle changes, better food choices, more consistent exercise, easier to sustain
- The North American Menopause Society’s 2022 position statement on hormone therapy notes its role in symptom relief and metabolic health during the menopausal transition (Menopause: The Journal of The North American Menopause Society, 2022)
The first thing that changed for me wasn’t my weight. It was my sleep.
A few weeks after starting the protocol my doctor recommended, I noticed I was waking up less during the night. Morning fatigue, the kind that used to sit on me for hours, started lifting earlier in the day. It took longer than I expected before the number on the scale reflected anything at all.
But once sleep improved, everything else I’d been trying, the food changes, the workouts, finally started to produce something. It wasn’t that the earlier effort had been wasted. It was that my body hadn’t been in a state where that effort could actually register.
The Framework: Four Things That Have to Work Together
Calorie restriction alone is a particularly weak strategy during menopause. It tends to burn through muscle as readily as fat, which lowers your metabolic rate further and makes the next round of restriction even less effective. What works instead is addressing the specific mechanisms driving the weight gain, together rather than one at a time.
Diet: Built Around Insulin and Muscle, Not Just Calories
- Preserves muscle against the accelerated loss described above
- A high-protein breakfast supports satiety hormones through the rest of the day
- Aim for 30–35g at breakfast specifically; it’s the meal most women shortchange
- Salmon, chicken, eggs, Greek yogurt, and cottage cheese are reliable sources
- Addresses insulin resistance at the source
- Swap refined carbohydrates for legumes, vegetables, and whole grains
- 25–35g of fiber daily supports blood sugar stability
- Steadier blood sugar means less of what you eat ends up as visceral fat
- Omega-3s from salmon, sardines, walnuts, and flaxseed
- Colorful vegetables, particularly berries and leafy greens
- Olive oil as your primary cooking fat
- A 12-hour overnight window (roughly 7pm to 7am) supports visceral fat reduction
- Larger meals earlier in the day, lighter dinners
- Finishing dinner 3 hours before bed supports both digestion and sleep

Exercise: Less Cardio, More Resistance
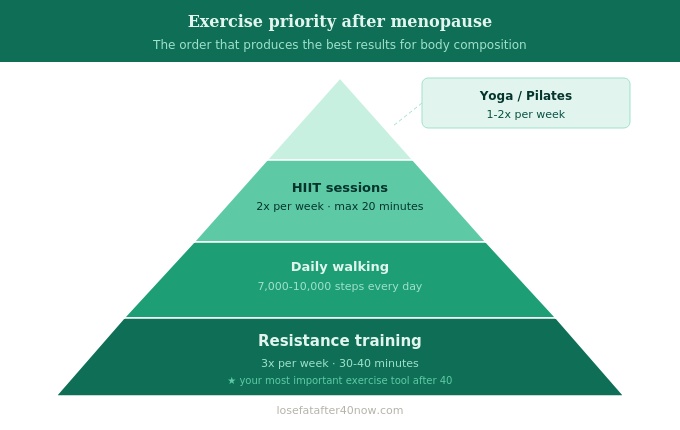
Exercise Priority After Menopause
- Resistance training, 3x/week, 30–40 minutes. The single most direct counter to the muscle loss driving menopause weight gain. It raises resting metabolic rate and improves insulin sensitivity at the same time.
- Daily walking, 7,000–10,000 steps. Doesn’t spike cortisol the way intense cardio can, and walking for 10 minutes after meals measurably softens the blood sugar spike that follows eating.
- HIIT, 2x/week, capped at 20 minutes. Efficient for insulin sensitivity without the sustained cortisol elevation that longer sessions can trigger.
- Yoga or Pilates, 1–2x/week. Lowers cortisol directly and supports the sleep quality that everything else depends on.
Long steady-state cardio sessions, 45 minutes or more, done frequently, chronically elevate cortisol. After menopause, without estrogen’s buffering effect, that translates fairly directly into abdominal fat storage. Shift the balance toward resistance training and walking, and treat longer cardio as an occasional addition rather than the main strategy.
Sleep: The Piece Everything Else Depends On
Sleep isn’t a footnote in this framework, it’s closer to the foundation. Night sweats and hormonal shifts fragment sleep architecture during the transition, and poor sleep independently worsens both insulin resistance and appetite regulation. A few habits make a measurable difference: keeping the bedroom cool, finishing your last meal several hours before bed, and treating a consistent wake time as seriously as a consistent bedtime.
Supplements Worth Discussing With Your Doctor
None of these fix menopause weight gain on their own. For me, they only became useful once sleep, protein intake, and consistent resistance training were already in place.
The most extensively studied herbal option for menopausal symptoms, working through serotonin pathways to reduce hot flash frequency. Better sleep from fewer night-time symptoms supports more stable hunger and fullness signaling the next day.
Activates AMPK and improves insulin receptor sensitivity, with several clinical trials showing modest weight-related effects. It can interact with certain medications, so this one is worth a direct conversation with your doctor before starting.
Involved in hundreds of enzymatic processes, including cortisol regulation and the pathway that supports sleep. Deficiency is common in women over 40 and can quietly compound several of the mechanisms above. A well-absorbed dose before bed is a reasonable starting point to discuss with your doctor.
Rich in gamma-linolenic acid, which supports the body’s inflammation-regulating processes. Commonly used for hot flashes and general hormonal comfort during the transition, with a gentler and slower onset than most other options here.
The biggest change in all of this wasn’t any single habit. It was what I check first thing in the morning.
I used to step on the scale before I’d even had coffee. If the number was up, the whole day felt heavier before it had really started.
Now the first thing I think about is whether I have a protein-forward breakfast planned, whether today includes a resistance session, how well I actually slept, and whether last night’s dinner was early enough. The scale still exists, but it’s stopped being the thing that tells me whether the day is going well. It’s become more like a monthly report on whether the rest of the system is actually working.
When to Consider GLP-1 Options
For women with significant insulin resistance, a BMI of 30 or higher, or menopause weight gain that hasn’t responded to sustained lifestyle changes, GLP-1 receptor agonists like semaglutide or tirzepatide have become an increasingly discussed option. Some clinical observations suggest combining these medications with hormone therapy may produce better outcomes than either approach alone, since estrogen’s role in insulin sensitivity may amplify how the body responds to both. This is a fast-moving area of research and a conversation to have directly with an endocrinologist or menopause specialist rather than something to self-direct.
Frequently Asked Questions
Is it actually possible to lose weight during menopause?
Yes, but general calorie cutting alone tends to underperform, because it burns through muscle as well as fat and lowers your metabolic rate in the process. What tends to work is targeting the specific mechanisms at play: insulin resistance through diet quality, visceral fat through resistance training and sleep, cortisol through stress management and shorter cardio sessions, and muscle preservation through adequate protein.
Why does belly fat feel different after menopause than it did before?
Because it typically is different. Post-menopause abdominal fat is predominantly visceral, sitting deep around the organs rather than just under the skin. It tends to feel firmer, and it doesn’t respond to exercise the same way subcutaneous fat does. Addressing it usually requires improving insulin sensitivity alongside staying active, not activity alone.
Should I talk to a doctor about menopause weight gain specifically?
A gynecologist or menopause specialist is generally a better starting point than a general practitioner for this particular issue. Worth asking about: your hormone levels, insulin and blood glucose markers, whether you’re a reasonable candidate for HRT, and current thinking on combining hormone therapy with GLP-1 medications if that’s relevant to your situation.
How long does the rapid weight-gain phase of menopause usually last?
The steepest gains tend to cluster in the two to three years surrounding the transition itself. After that window, weight can keep climbing more slowly unless it’s actively addressed, and the shift toward visceral fat distribution generally doesn’t reverse on its own without some combination of the strategies above.
Do the same strategies that worked for weight loss in my 30s still apply now?
Often not, because the underlying mechanisms have changed. Calorie counting that worked at 35 tends to cost you muscle now rather than fat. Cardio that worked then can raise cortisol in ways that work against you now. The approach that tends to hold up is built around protein, resistance training, sleep, and directly addressing insulin resistance, rather than the strategies you relied on a decade earlier.
The Bottom Line
Those 11.4 pounds between 43 and 45 weren’t a sign that I’d stopped trying. They were the visible result of several biological changes happening at once, changes I didn’t have a name for yet and wasn’t equipped to address with the tools I’d always relied on.
What actually shifted things wasn’t more restriction or more mileage. It was more protein, more resistance training, earlier dinners, and, more than anything, treating my sleep as seriously as I treated my workouts. None of it moved quickly, and none of it was a straight line.
But the direction changed. Understanding why my body was responding this way turned what had felt like failure into something closer to information, and information is something you can actually work with.
What was the first thing that shifted for you once you understood what your body was actually doing? I read every comment, and your experience may be exactly what someone else needs to hear right now.
Medical Disclaimer: This post is for informational purposes only and does not constitute medical advice. Please consult your healthcare provider before making changes to your diet, exercise, or supplement routine, and before considering hormone therapy or GLP-1 medications.




