How Intermittent Fasting Changes After Menopause
Intermittent fasting after menopause had never been something I thought I’d need to reconsider — until it stopped working the way it used to.
For several years from the time I was 47, the same protocol had run reliably in the background of my days. Sixteen hours of fasting, eating between noon and eight in the evening. Black coffee to carry me through the mornings. I didn’t fight it. My energy held steady during fasting hours. Sleep wasn’t a concern.
Sometime in my early 50s, that changed.
The edginess arrived first. Around 10 AM, during what should have been an unremarkable fasting morning, I felt a low-level irritability I couldn’t quite trace. Not hunger, not fatigue — something more like background tension that made small things harder to brush past. I’d find myself reacting to things I would normally have let go entirely.
The nights gave me the clearest information. When I’d eaten early and lightly, exactly as I had at 47. I couldn’t settle. I’d lie in bed tense and wired, exhausted but unable to rest. Sleep came in fragments. I’d wake in the middle of the night, mind active, body unable to fully let go. Mornings arrived and I hadn’t really recovered.
When I tested a simple adjustment — cutting the fasting window back to around 14 hours, and adding more protein and healthy fat to dinner rather than keeping it light. The nights calmed down within a few days. The morning edginess eased within about two weeks.
That response told me something specific. Intermittent fasting after menopause isn’t something to abandon. But the hormonal terrain it operates in has shifted in ways that standard 16:8 advice doesn’t account for. Understanding what actually changed, and what to do about it, is what this post covers.

Something Changed, and It Wasn’t Your Discipline
The experience I described above is one that many post-menopausal women encounter when they continue an IF protocol that worked during their 40s. The fasting window that once felt almost effortless starts requiring real push-through. The mornings feel harder. Sleep, which often improves with IF initially, begins to fragment again.
The typical response is to hold the protocol. Keep the window. Trust the process. And for some women, this works. But for others, holding a protocol that isn’t matched to the post-menopausal hormonal environment quietly makes things worse: more cortisol, worse sleep, more of exactly the pattern that drives post-menopausal belly fat accumulation in the first place.
The reason this is specific to intermittent fasting is that IF is fundamentally a hormonal intervention. It works by manipulating insulin and cortisol through timing. When the hormonal context those mechanisms operate in changes significantly (as it does after menopause), the same timing produces different outcomes.
Menopause isn’t just a drop in one hormone. It’s a reorganization of the entire endocrine system, and the effects of that reorganization matter for how fasting works in the body.
What Actually Shifts in Your Body After Menopause
To understand why IF needs adjusting, it helps to be specific about what the hormonal landscape actually looks like after your final period.
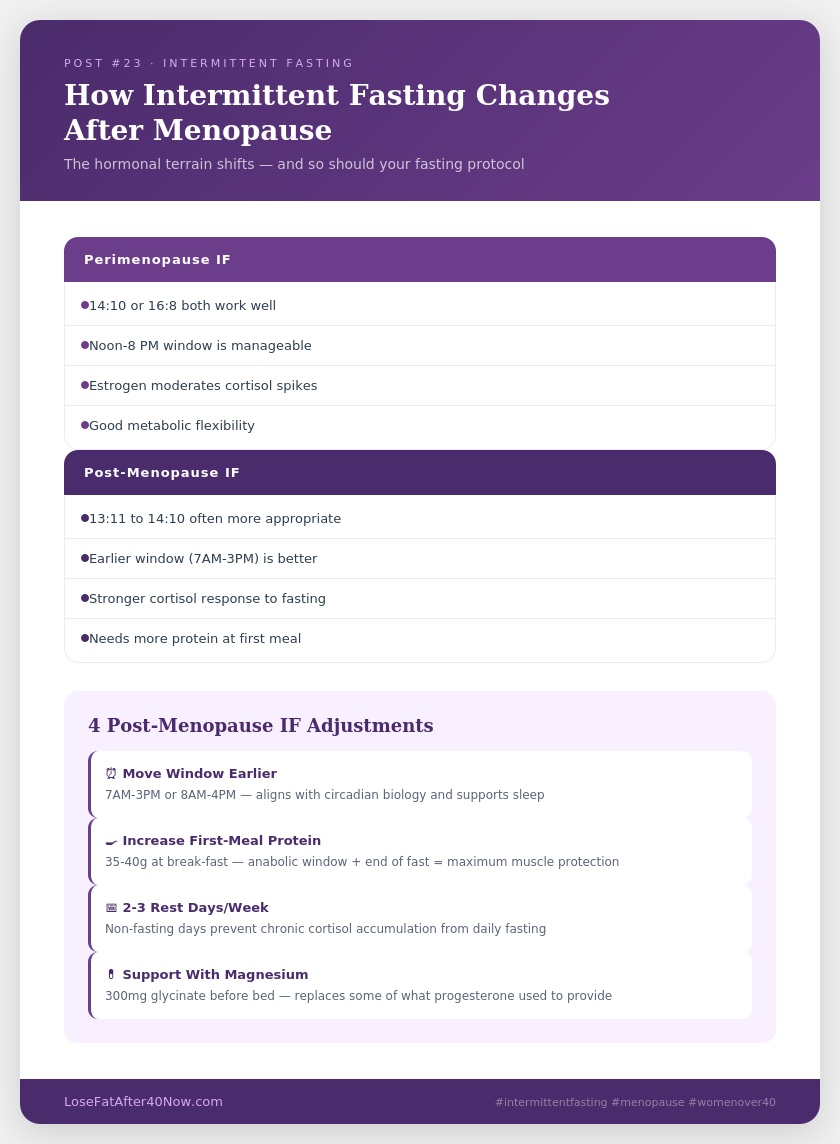
Estrogen settles at a permanently lower level. During perimenopause, estrogen fluctuates unpredictably. After menopause, it stabilizes at a consistently reduced baseline. Estrogen had been doing significant work behind the scenes: supporting insulin sensitivity, buffering the cortisol stress response, moderating appetite signals. All of that support is now consistently absent.
Progesterone drops to near zero. Progesterone is a GABA receptor agonist that promotes the brain’s primary calming mechanism. Its near-complete absence after menopause has direct consequences for sleep quality, stress resilience, and the body’s ability to recover from physiological stressors, including the mild stress of fasting (Journal of Clinical Endocrinology & Metabolism, 2018).
The cortisol stress response runs hotter. With both estrogen and progesterone no longer moderating the HPA axis (the system governing cortisol release), the body’s response to physical and emotional stressors becomes more pronounced and lasts longer. Fasting is a mild physiological stressor. Post-menopause, the cortisol response to that stressor tends to be stronger and slower to clear than it was before (Psychoneuroendocrinology, 2020).
Insulin resistance increases further. Post-menopausal insulin resistance often worsens beyond what occurred during perimenopause. This is the primary driver of the visceral fat accumulation that characterizes the post-menopausal decade. Managing blood sugar and insulin becomes both more important and more challenging.
Post-Menopause Metabolism: What the Research Shows
For a broader overview of how these hormonal changes interact with overall health, the National Institute on Aging’s menopause overview provides useful context on the metabolic and hormonal shifts that matter for dietary strategies like intermittent fasting.
Why Intermittent Fasting After Menopause Hits Differently
I didn’t connect my symptoms to my fasting protocol immediately. What I noticed first was that something about my daily rhythm had gotten harder: not the hunger, but the emotional texture of the fasting hours.
On mornings when the overnight fast had been long or I’d kept dinner very light the night before, the fasting hours felt wrong in a specific way. Tense before I could identify why. Easily rattled by things that would have rolled off before. In my late 40s, the same protocol had left me feeling clear. In my early 50s, the same hours left me on edge.
The sleep connection took a few weeks to recognize clearly. The worst nights were after lighter, earlier dinners. I’d wake somewhere between 2 and 4 AM, mind active, body tense, unable to drift back down for a long stretch. Nights after a more substantial dinner with protein and healthy fat were noticeably calmer, even if not perfect.
Once I understood the mechanism, this made complete sense. Without progesterone’s calming effect and without estrogen’s cortisol buffer, the fasting state (a mild stress state by definition) produces a stronger cortisol elevation in post-menopausal women. That elevation, when it extends through the overnight hours, directly disrupts sleep architecture. And disrupted sleep creates more cortisol the following day, which makes the next fasting window harder. The cycle compounds.
There is also the specific question of the early morning. Cortisol is naturally highest immediately after waking, known as the cortisol awakening response.. When there is no food to signal safety after that morning cortisol peak, the elevation can linger significantly longer without estrogen moderating the descent. This is why fasting mornings feel qualitatively harder for many post-menopausal women than the same hours did a decade earlier. The hunger is manageable. The mood and stress response are what shift.
How the Post-Menopausal Hormonal Shift Changes the Fasting Experience
- Cortisol response to fasting is stronger without estrogen buffering the HPA axis, fasting produces a more pronounced cortisol elevation that takes longer to clear (Psychoneuroendocrinology, 2020)
- Morning cortisol lingers longer the cortisol awakening response peaks higher and descends more slowly without estrogen’s moderating effect, making early fasting hours harder
- Sleep disruption compounds the problem fragmented overnight sleep elevates the next day’s cortisol, which makes subsequent fasting windows progressively more difficult
- Progesterone absence reduces overnight recovery without GABA support from progesterone, the nervous system is less able to fully downregulate during sleep (Journal of Clinical Endocrinology & Metabolism, 2018)
The Metabolic Case for IF After Menopause Is Stronger Than You Think
Given the challenges described above, it might seem like intermittent fasting after menopause creates more problems than it solves. The opposite tends to be true: the reasons to practice some form of time-restricted eating become more compelling post-menopause, not less.
The central metabolic challenge after menopause is insulin resistance. Estrogen had been supporting insulin sensitivity throughout the reproductive years. With its consistent decline, post-menopausal women face a meaningful worsening of insulin response that affects how carbohydrates are processed, where fat is stored, and how efficiently the body clears glucose after meals.
Intermittent fasting works directly on this problem. By extending the periods during which insulin levels remain low, time-restricted eating gives the body regular windows to recover insulin sensitivity, access stored fat, and reduce the visceral accumulation pattern that drives post-menopausal metabolic risk. Research consistently confirms this effect specifically in post-menopausal women: a 2022 study found that time-restricted eating produced greater reductions in insulin resistance and visceral fat than standard caloric restriction alone, over 12 weeks (Obesity, 2022).
Autophagy (the cellular cleanup process triggered by extended fasting) also becomes more valuable with age. The cellular maintenance that comes with 14 or more fasting hours matters more, not less, as the body’s natural repair systems slow down over time.
The goal of adapting the protocol isn’t to get the benefits of intermittent fasting after menopause with less effort. It’s to get the same benefits without triggering the cortisol and sleep disruption that an ill-fitting protocol produces.
Three Reasons to Keep Fasting After Menopause
- Insulin resistance is the core post-menopausal metabolic challenge and TRE directly addresses it by extending low-insulin windows each day
- Visceral fat responds to TRE research shows greater visceral fat reduction with time-restricted eating than with caloric restriction alone in post-menopausal women (Obesity, 2022)
- Autophagy becomes more valuable, not less the cellular repair triggered by 14+ hour fasting windows compounds in benefit over time, supporting healthy aging at the cellular level
How to Rebuild Your IF Protocol for the Post-Menopause Body
The adjustment I made wasn’t dramatic. I didn’t overhaul everything at once. I started with the smallest change that seemed most likely to explain the sleep problem, and worked from there.
My first step was shortening the fasting window. Rather than holding 16 hours daily, I moved to around 14 hours on most days. On days when I hadn’t slept well or had something demanding ahead, I allowed myself to ease back to about 12 hours, eating a lighter breakfast earlier without making it a formal part of the protocol, just a practical acknowledgment of what the body needed that day.
I also changed what I ate at dinner. Where I’d kept dinner quite light — the idea being that eating less in the evening extended the next day’s fasting window more cleanly. I added protein and healthy fat back in. Not a heavy meal, but enough to give the body resources to work with overnight. This was the change that made the most immediate difference to my sleep. Within a few days, the middle-of-the-night waking became less frequent. Within a couple of weeks, the morning edginess had eased considerably, and the sharp, sudden hunger that had been hitting unpredictably was much less intense.
I also became more honest about rest days. Two or three days a week where I simply ate three balanced meals at natural times, without tracking the fasting window at all, reduced the cumulative cortisol load while preserving the metabolic benefits of the fasting days. This isn’t failure. It’s a deliberate part of the protocol.
The goal of rebuilding intermittent fasting after menopause isn’t to do less. It’s to work with the hormonal reality of the post-menopausal body rather than against it.
| Adjustment | What to Do | Why It Matters Post-Menopause |
|---|---|---|
| Shorten the window | 16:8 → 14:10; allow 12:12 on difficult days | Reduces cortisol load from extended fasting while preserving insulin and autophagy benefits |
| Move the window earlier | First meal by 7–8 AM; close eating window by 4–6 PM when possible | Aligns eating with insulin sensitivity peaks; supports cortisol descent and melatonin rise for sleep |
| Strengthen dinner with protein | 35–40g protein + healthy fat at the evening meal | Reduces overnight cortisol elevation; supports sleep quality in the absence of progesterone |
| Add non-fasting days | 2–3 days per week: 3 balanced meals, no timing restriction | Prevents chronic cortisol accumulation; protects HPA axis regulation over time |
| Protein at your first meal | 35–40g protein to break the fast | Maximizes muscle protein synthesis window; blunts the post-fast cortisol spike |
The Early Eating Window Advantage

The most significant structural shift for post-menopausal women is moving the eating window earlier in the day, what researchers call early time-restricted eating (eTRE),.
Insulin sensitivity follows a circadian rhythm. The body is most efficient at processing carbohydrates and managing blood sugar in the morning, and progressively less efficient as the day goes on. A post-menopausal woman eating the same foods at 8 AM and at 8 PM will experience meaningfully different insulin responses. The morning meal is handled more cleanly, with a smaller and shorter insulin spike, less visceral fat signal, and faster glucose clearance.
Cortisol is naturally highest in the first hours after waking, designed to peak and then descend through the day. Eating breakfast signals safety to the body and supports that cortisol descent. Eating well into the evening (the pattern reinforced by the traditional noon-to-8 PM window) works against the natural cortisol curve and can suppress melatonin production, making sleep onset harder.
Research confirms that shifting the eating window earlier produces metabolic benefits that go beyond fasting duration alone. A 2019 study found that eating within an earlier time window improved insulin sensitivity, blood pressure, and oxidative stress markers independently of caloric intake; the timing itself was doing measurable metabolic work (Cell Metabolism, 2019).
The practical implication: shifting your window earlier, even if you don’t shorten it significantly, may provide more benefit for the post-menopausal body than extending the fast while keeping the window late.
Sample Early Eating Window Schedule (Post-Menopause)
- 7:00–8:00 AM: First meal: 35–40g protein, moderate healthy fat, some complex carbohydrate
- 12:00–1:00 PM: Second meal: protein, generous vegetables, healthy fat
- 3:00–5:00 PM: Third meal (lighter): protein, vegetables, minimal carbohydrate
- From 5:00–6:00 PM: Fasting window begins; herbal tea and water only
- Fasting window length: 13–15 hours, adjusted based on the previous night’s sleep quality and the day’s stress level
Signs It’s Time to Adjust Your IF Protocol
If you are post-menopausal and currently practicing intermittent fasting, honest self-assessment is more useful than strict protocol adherence. These are the signals that typically indicate the current approach needs modification. Three or more consistently present is a clear signal to act; more willpower is not the answer when the issue is a hormonal mismatch.
When Your IF Protocol Needs Post-Menopause Adjustment
- Sleep quality has gotten worse since continuing the protocol, especially waking between 2 and 4 AM
- Fasting mornings feel emotionally harder than they used to: irritability, anxiety, or difficulty managing reactions
- Hunger feels urgent and sharp rather than gradual and manageable
- Energy during fasting hours is lower than when you started, rather than improving over time
- Hair thinning has accelerated since beginning or continuing the protocol
- Body composition is not improving despite consistent adherence and good food choices
- You feel noticeably better on non-fasting days than on fasting days, consistently
Any three of these appearing together is a strong signal to shorten the window, move it earlier, or build in regular non-fasting days. The body is giving specific, useful information.
Frequently Asked Questions
Does intermittent fasting help with weight gain after menopause?
Yes, particularly with the insulin resistance that drives most post-menopausal weight gain. Research consistently shows that time-restricted eating improves insulin sensitivity and reduces visceral fat in post-menopausal women, with greater effect than caloric restriction alone. The key is adjusting the protocol to match the post-menopausal hormonal environment: a shorter window, earlier timing, and adequate protein at dinner to support overnight cortisol regulation.
Is intermittent fasting safe after menopause if I have osteoporosis concerns?
This requires individual guidance from your healthcare provider. Bone density concerns interact with dietary patterns in ways that vary significantly between individuals. If you have significant bone health concerns, discuss any major changes to your eating schedule with your doctor before starting or adjusting an IF protocol.
What is the best fasting window length for post-menopausal women?
There is no single answer, but 13 to 14 hours tends to offer meaningful metabolic benefits while reducing the cortisol load of longer fasts. A practical starting point: finish dinner by 7 PM and break the fast at 8 AM, creating a 13-hour window. Assess sleep quality, morning mood, and hunger patterns over 2 to 3 weeks before adjusting further. These three signals give faster, more honest feedback than the scale.
Does the timing of the eating window matter as much as the length?
Research increasingly suggests that timing matters significantly, not just fasting duration. Aligning the eating window with the morning and early afternoon, when insulin sensitivity is highest, produces better metabolic outcomes than the same fasting hours with a late eating window. For post-menopausal women specifically, moving the window earlier may be the single most impactful adjustment available.
Does HRT affect how intermittent fasting works after menopause?
Women on hormone replacement therapy may find their fasting tolerance is closer to the perimenopausal pattern, because HRT restores some of the hormonal context that makes longer windows more manageable. The early eating window advantage appears to hold regardless of HRT status, but the cortisol sensitivity to extended fasting may be less pronounced for women on appropriate HRT. Individual responses vary; sleep quality and morning mood remain the most useful feedback signals regardless.
What to Start With
The shorter window is not a compromise. Adding protein to dinner is not a workaround. These are adaptations to a body that has legitimately different hormonal needs than it did five or eight years ago, needs that the standard 16:8 framework was not designed to accommodate.
The most useful starting point isn’t changing the window length or shifting the timing. It’s watching sleep quality and morning mood first. When intermittent fasting after menopause is working for the body rather than against it, nights become calmer. Mornings feel clearer. The edginess that signals elevated cortisol eases. Appetite becomes more predictable. The scale tends to follow, but sleep and mood tell you sooner and more honestly whether the protocol is helping.
Intermittent fasting after menopause remains one of the most effective strategies available for managing insulin resistance and the visceral fat pattern that comes with it. Getting the protocol right for your current hormonal reality is what makes the difference between a tool that helps and one that quietly adds to the cortisol load your body is already managing.
Have you noticed your experience with intermittent fasting shifting since going through menopause? What adjustments have made the biggest difference for you? I’d love to hear in the comments below.
Disclaimer: This post is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before making significant changes to your diet or eating schedule, especially if you have existing health conditions, concerns about bone density, thyroid function, or are considering hormone-related dietary strategies.